
Not All That Consolidates Is Cancer: A Case of Diesel-Induced Lipoid Pneumonia Masquerading as a Mass
- Post by: admin
- April 22, 2025
- No Comment
Dr Dwijen Das1 Dr Sweekriti Adhikari2 Dr Ranjit Ray3 Dr Sumi Dutta4 Dr Prapti Gogoi5
Professor and HOD1 Assistant Professor2 Post Graduate Trainee3,4,5
Abstract
Exogenous lipoid pneumonia is an uncommon pulmonary condition caused by the aspiration or inhalation of lipid substances. We report a rare case of lipoid pneumonia in a 50-year-old male following accidental ingestion of diesel. The patient presented with shortness of breath, dry cough, and pleuritic chest pain. Imaging revealed classic features including consolidation and fat density in the lungs. He was managed successfully with corticosteroids and demonstrated clinical improvement. This case highlights the importance of recognizing lipoid pneumonia in the differential diagnosis following hydrocarbon exposure.
Keywords
lipoid pneumonia, diesel ingestion, hydrocarbon pneumonitis, exogenous lipid pneumonia, corticosteroids
Introduction
Lipoid pneumonia is a rare form of pneumonia resulting from the accumulation of lipid substances in the lungs. It is classified as either exogenous or endogenous depending on the source of the lipid. Exogenous lipoid pneumonia typically results from aspiration or inhalation of oily substances, such as mineral oil, petroleum jelly, or hydrocarbons like diesel fuel (Bandla, Davis, & Hopkins, 2011). Diesel ingestion is a particularly uncommon cause and can lead to significant respiratory complications. Early diagnosis is crucial to prevent long-term pulmonary sequelae.
Case Presentation
A 50-year-old male with no prior comorbidities presented to the emergency department with progressive shortness of breath, dry cough, and right-sided pleuritic chest pain for two days. The symptoms developed following accidental ingestion of approximately 100 mL of diesel while siphoning fuel.
On examination, the patient was alert and hemodynamically stable with an oxygen saturation of 94% on room air. Respiratory examination revealed coarse crepitations over the right lower lung zones. The rest of the systemic examination was unremarkable.
Imaging
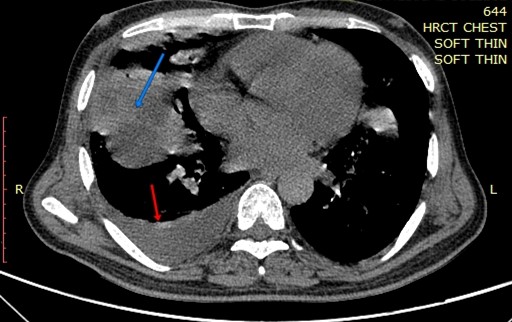
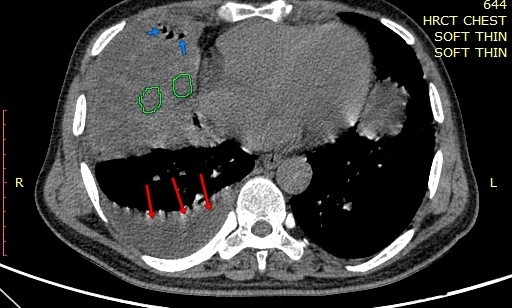
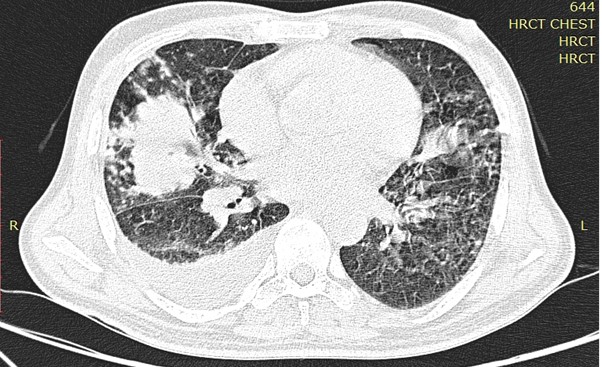
A chest radiograph showed consolidation in the right middle lobe. High-resolution computed tomography (HRCT) of the thorax revealed consolidation with air bronchograms and regions of fat attenuation within the lesion, which are hallmark features of exogenous lipoid pneumonia along with moderate right side pleural effusion. (Marchiori et al., 2011).

Management
The patient was managed with intravenous methylprednisolone 500 mg daily for three days. He showed significant clinical improvement during hospitalization. A follow-up chest imaging was advised after six weeks to assess radiologic resolution.
Discussion
Exogenous lipoid pneumonia is most often seen in individuals who aspirate oil-based substances, whether due to traditional remedies, occupational exposure, or accidental ingestion. Hydrocarbons like diesel are particularly hazardous due to their low viscosity and high volatility, allowing deep penetration into the pulmonary tree (Cottin et al., 1999).
Imaging plays a crucial role in diagnosis. Chest radiographs may show alveolar infiltrates, typically in the dependent lung zones. HRCT is more definitive, often revealing areas of consolidation with low attenuation values due to fat content, as seen in our patient (Marchiori et al., 2011).
Bronchoalveolar lavage (BAL) can aid in diagnosis by demonstrating lipid-laden macrophages; however, in our case, the diagnosis was established based on clinical and radiologic findings. Treatment is largely supportive. The use of corticosteroids remains controversial but has shown benefit in reducing inflammation and hastening clinical recovery in several reported cases (Hadda & Khilnani, 2010).
Our patient responded well to a short course of intravenous corticosteroids, with symptomatic improvement. He was discharged with outpatient follow-up and advised for repeat imaging.
Conclusion
Exogenous lipoid pneumonia should be considered in patients presenting with respiratory symptoms following diesel or hydrocarbon exposure. Timely imaging and supportive management, including the judicious use of corticosteroids, can lead to favorable outcomes. Awareness of this condition is vital for clinicians to avoid misdiagnosis and unnecessary treatment.
References
Bandla, H. P., Davis, S. H., & Hopkins, N. E. (2011). Lipoid pneumonia: A silent complication of mineral oil aspiration. Pediatric Radiology, 41(5), 643-645. https://doi.org/10.1007/s00247-010-1914-0
Cottin, V., Gary, G., Reynaud-Gaubert, M., & Cordier, J. F. (1999). Exogenous lipoid pneumonia: A retrospective multicentre study of 44 cases in France. European Respiratory Journal, 14(2), 356-359. https://doi.org/10.1034/j.1399-3003.1999.14b13.x
Hadda, V., & Khilnani, G. C. (2010). Lipoid pneumonia: An overview. Expert Review of Respiratory Medicine, 4(6), 799-807. https://doi.org/10.1586/ers.10.57
Marchiori, E., Zanetti, G., Mano, C. M., & Hochhegger, B. (2011). Exogenous lipoid pneumonia: Clinical and radiological manifestations. Respiratory Medicine, 105(5), 659-666. https://doi.org/10.1016/j.rmed.2010.12.012